Your broken hip
This page has been written to help you have a better understanding of the treatment you require because your hip bone has broken. In hospital we describe a broken bone as a fracture.
Why operate?
A hip fracture is a very painful injury. Our aim is to reduce your pain and make sure you make the best recovery possible.
Without surgery you would be unable to leave your bed for 3 months which would put you at risk of many complications. The most common and serious complications are; chest infections leading to pneumonia and pressure sores. Many people find after a long period in bed that they are unable to walk again.
Having surgery to fix the bone is the most common treatment for this injury. Surgery will reduce your pain and enable you to begin physiotherapy and return to mobility as quickly as possible.
Types of surgery
There are 2 types of hip fracture operations which are routinely used to treat the broken bone. The decision on which is most suitable for you will depend on where the break is.
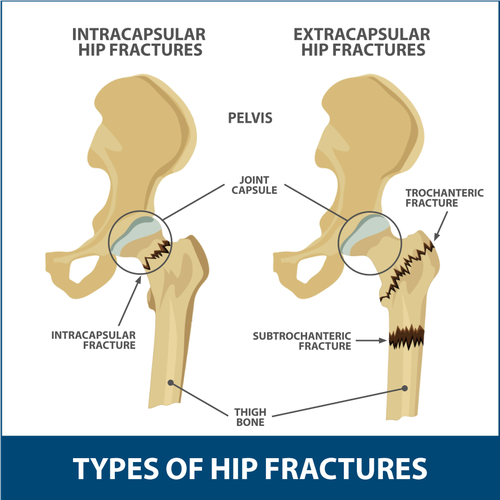
Intracapsular Hip Fracture
This is a common place to break your hip and because the capsule supplies blood to the bone, it will not repair itself. Therefore, it is fixed with a metal device which is known as hemiarthroplasty.
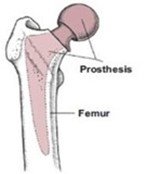
Hemiarthroplasty
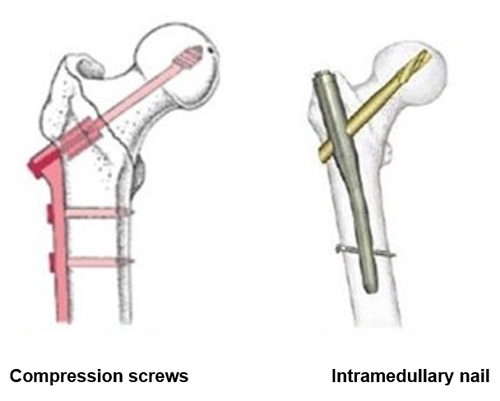
Extracapsular Hip Fracture
This is when the break is outside the capsule and the blood flow to the bone has not been damaged. This is repaired either with a plate and screws (Dynamic Hip Screw or DHS) or with a nail down inside the femur and screws up into the head of the femur.
Your surgeon will discuss with you the best options for the type of break you have.
How long until I am back on my feet?
We want to get you mobile as quickly as possible. Most patients are sitting out in a chair the day after their surgery.
Gradually, with the help of the therapists you will do more on your feet until you are fit enough to leave hospital. Some people may need a period of rehabilitation in a Community Hospital if they find they are still unsteady on their feet.
Most people are in Gloucestershire Royal Hospital for about 10 days. Some patients need much longer, while younger fitter people go home after about 5 days.
It is common for patients to compare themselves to others around them but please do not expect everyone to recover in the same way. If you have broken your hip, your recovery will take longer than friends and family who have had planned surgery.
We will ask your relatives to bring in some day clothes so that you will be more comfortable sitting out in a chair. We will also ask your relatives to fill in a form with the height of your furniture at home. This is so that we can supply equipment for your family to adjust, to make living at home as easy and safe as possible for you. We may do a home visit if it is felt necessary.
What to expect
As soon as the Emergency Dept (ED) confirm you have broken your hip, they will give you an injection in your groin to block the nerve to the hip to reduce the pain. You will then be referred to the Orthopaedic team (bone doctors). The Orthopaedic team will see you either in ED or on the ward and will discuss with you the treatment plan. They will examine you and ask you a short series of memory questions.
The team
On the ward you will also meet the Orthogeriatric team. This team of doctors work to make sure that you are as well as possible before your operation. They will also arrange other investigations if required. The Orthogeriatric team will continue to look after you after your operation, until you are fit to go home.
You will also be seen by the anaesthetist and theatre staff, the therapy team and a nutritionist. You will meet the porters, the X ray team, the domestic staff and the volunteers – care is shared between a large team of people working to get you better, and is very much a joint venture with you, to get you well again.
The surgery
We will do the operation as soon as we can - often the next day, but there may be a delay if you are physically not well enough, if the appropriate surgeon is not available or if there are other emergencies who need to be treated immediately.
Possible complications from having an operation
Repair of a hip fracture is considered as major surgery and has some common complications which are:
Delirium
Out of every 10 patients, we expect that 4 or 5 will become a bit muddled after surgery. This can involve forgetting where you are and what is happening, having vivid dreams that you are somewhere else or that people are behaving strangely. This is particularly common if you have had some memory issues beforehand. We will try and minimise the risks by using lower risk medications and making sure you can see and hear things properly. Delirium often settles after a few days but may take longer for you to feel back to your usual self.
Urinary retention
Many people find it difficult to use a bottle or bed pan in bed. We try to avoid putting in a catheter to drain your urine but if you cannot pass urine naturally, it may be necessary.
Constipation
Constipation is a risk from not eating, not moving around and from some pain relief medication. We will give you regular laxatives until your bowel pattern is back to normal.
Blood transfusion
About 1 in 4 of our patients need a blood transfusion after surgery as bones do bleed a lot.
Deep Vein Thrombosis (DVT)
Being immobile and having an operation leads to an increased risk of blood clots forming in your legs which may break off and lodge in your lungs. We will give you an injection in your abdominal wall each day to reduce the risk of this happening, unless you are on blood thinning tablets. You will continue to have these injections for 28 days after the operation, even if you leave hospital sooner.
Wound problems
Sometimes the wound will leak blood or clear fluid. Often this settles by itself or with a special dressing. You will need to stay in hospital until the wound stops leaking because of the risk of infection.
Loss of mobility
A hip fracture is a serious injury. Although we aim to get you back to your previous standard of mobility, about half of people who have had a hip fracture operation may newly need a stick or a frame to help with their mobility. About 10 in every 100 of our patients will need a new placement in a care home.
Death
Most of those people who sustain a hip fracture are very frail and elderly or reaching the end of their natural lives. About 6 in every 100 people will die during their hospital stay (not usually during the operation), and 30 in every 100 patients will die within one year of fracturing their hip.
Other assessments
While you are in hospital, we will ask about other falls you may have had. We will take your blood pressure lying down and standing up to see if it varies. We may also test your vision and assess your need for walking aids.
We will ask about risk factors for thin bones (osteoporosis). We may decide on treatment to strengthen your bones, or if you are younger, we will perform a bone density (DXA) scan.
Frequently asked questions
Can my relatives see a doctor?
The doctors are generally busy with ward rounds in the mornings and may not have time to stop and talk at length. Often the nurses will know what is happening and will be able to update your relatives on your progress if they ask.
The medical team are also happy to see families, particularly in the afternoons but at other times by arrangement - please ask your family to leave a phone number with the ward clerk and we will find a mutually convenient time to see them or give them a ring. We will of course let your family know if we are particularly concerned about anything.
Can I have a shower or bath?
You will be able to have a shower a week after the operation, if the nurses are happy with the wound. You should pat the wound area dry and cover with a new dressing. You should aim to keep the wound covered for about 2 weeks and then leave it open to the air. Showers are better than baths at not getting the wound soggy until it has healed. If needed, we will give you some spare dressings to take home.
Are there clips or stitches to be taken out?
Most surgeons will use dissolving sutures (stitches) or glue. The nurses will tell you if there are stitches or clips which will need to be taken out at 10 to 14 days. The Community Nurse can do this at home and will contact you to arrange, if needed.
Can I drive again?
You need to avoid driving for 6 weeks after the operation – longer if you do not feel fully confident in the strength of your leg.
Will I be seen in outpatients?
Most patients do not need to be seen again at the hospital.
Some patients need to be seen if they have had a total hip replacement or if there is something unusual about the surgery. The surgeons will let you know if this is the case.
Contact information
Further information
Royal Osteoporosis Society
Website: www.theros.org.uk