Having a therapeutic gastroscopy as an outpatient
You have been advised to have a therapeutic gastroscopy which provides treatment carried out via an endoscope. A gastroscopy may also be referred to as an endoscopy or OGD (meaning an oesophageal-gastroduodenoscopy).
It is important that you read this page before your appointment so that you understand the procedure and the preparation involved.
If you have diabetes and you are receiving treatment please leave a message on the Medication Advice Line (the number is at the end of this page). A member of staff will return your call normally within 24 hours, week days only.
If you are using an insulin pump we would like your BM to be 7mmol/L. Please call your local pump team if you need further advice.
If you are taking any medication that thins your blood other than aspirin (which you can continue to take) please contact the Medication Advice Line.
This is very important as your procedure may be delayed if you do not get advice.
If required, you may be asked to attend the radiology department for imaging tests on the same day as your gastroscopy.
What is a gastroscopy?
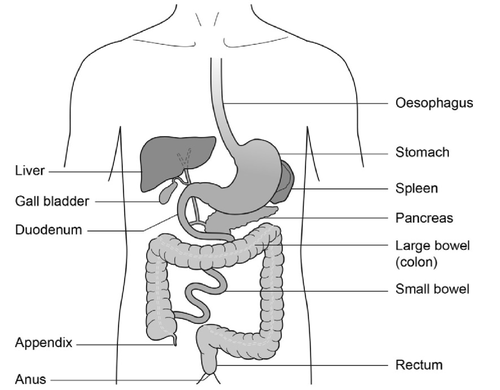
Gastroscopy is an investigation to look directly at the lining of the oesophagus (gullet/food pipe), the stomach and around the first bend of the small intestine (the duodenum). A gastroscope is passed through the mouth, down the oesophagus and into the stomach.
A gastroscope is a long flexible tube, thinner than your little finger. It has a bright light at the end (this is not hot), which is necessary to be able to see the lining of the stomach.
Pictures are transmitted on to a screen.
There are a variety of therapeutic procedures that can be performed endoscopically. The following information provides explanations for all therapeutic procedures; your doctor will have already explained the therapy that you require.
Dilatation
A dilatation can be performed if a narrowing of the food pipe (oesophagus) is found. This means stretching the narrowing to improve your swallowing. Usually the need for this procedure has been identified on a previous gastroscopy.
Banding
Banding is a way to treat oesophageal varices. These are like varicose veins in your oesophagus. The endoscopist will place special elastic bands around each of the varices. This stops the blood supply to these veins and they will eventually disappear. This will not affect the normal blood supply to the oesophagus.
If you have been diagnosed with oesophageal varices you will normally be on a surveillance programme and the endoscopist will decide how often you will need this done.
EMR (Endoscopic Mucosal Resection)
EMR is a minimally invasive, safe and well established method of removing polyps. An endoscope is introduced to the site of the polyp. Using a small needle, which is passed through the channel on the endoscope, a fluid is injected underneath to raise the polyp above the intestinal lining therefore creating a safe field to remove it.
A metal snare will be placed around the polyp and a small amount of current will be passed through to cut the polyp while cauterising (sealing) the blood supply.
If the polyp is large, the above steps may need to be repeated until it is completely removed. Metal clips may be placed, after the removal, at the wound site to assist with healing and to prevent complications. The polyp will be sent for analysis under the microscope.
RFA (Radio Frequency Ablation)
RFA involves introducing high frequency radio waves directly into a small area of tissue to destroy or ablate (remove).
This technique has been developed specifically to destroy the abnormal cells in the lining of the oesophagus. These cells look different so they can be easily recognised in an endoscopy examination. This is called Barrett’s oesophagus which is caused by acid reflux changing the cells in the lining of the oesophagus. A small balloon is introduced into the area of abnormal cells and high intensity radio waves are passed through it. This causes intense heat, but only in the region very near to the surface of the balloon. The abnormal cells are killed, but the normal non-Barrett’s cells nearby are left unharmed. After treatment, not only are the precancerous cells (dysplasia) removed, but the entire Barrett’s oesophagus segment is removed as well.
Most patients require 2 or 3 treatments over a period of a few months. A small number of patients may need more treatments.
Sometimes, radiofrequency ablation needs to be combined with Endoscopic Mucosal Resection (EMR) if the surgeon sees visible nodules (swellings) in the lining of the oesophagus.
Botulinum toxin injection
Botulinum toxin can be injected directly into the muscle of the oesophageal wall. This is given for a condition in which the muscles of the lower part of the oesophagus fail to relax preventing food from passing into the stomach. This is called achalasia. The toxin paralyses the muscle and this effect can improve symptoms although the effects are not permanent, further injections are typically given as and when required.
Stenting
An oesophageal stent is an expandable tube made of a flexible metal which allows it to expand over a period of hours. This will make it easier for you to swallow food and fluids. Your consultant will choose the right stent and size for your needs. This procedure is carried out with X-ray to ensure the correct placement of the stent.
Please note that none of the procedures mentioned in this section are available at Stroud or Cirencester Hospitals.
Preparing for your procedure
To allow a clear view during the procedure the stomach must be completely empty. You are therefore asked not to have anything to eat for at least 6 hours before your appointment time. You may have sips of water up to 2 hours before your appointment time.
You are advised not to wear expensive items of jewellery or clothing when you visit the Endoscopy Unit.
The NHS, a major contributor of carbon emissions in the UK, has recently outlined ambitious targets to achieve net zero carbon emissions by 2040. The endoscopy team in Gloucestershire have carefully considered ways of adopting more sustainable care and waste reduction. We would appreciate your support to help make our practice ‘greener’ by kindly bringing the following items along to your endoscopy appointment, so that single use alternatives are not required:
- If applicable, your own denture pot, hearing aid case(s) and/or eye glasses case
- Water bottle
- Reusable cup with lid for a complimentary hot drink after the procedure
On admission
On arrival at the department you will be seen by a nurse who will check your personal details.
You will be asked a series of questions about any operations or illness that you may have had or are presently suffering with.
Please bring a list of all medications you are currently taking.
The nurse will also ask if you have any allergies or reactions to medicines or foods.
You might also be given a small dose of Parvolex® and Infacol®, by mouth, to reduce the secretions in your oesophagus and bowel. It will also give a better view of your oesophagus and stomach during the procedure. Please do not have any other liquids after you have been given the Parvolex® and Infacol® - the nurse giving you this medication will also remind you not to have any further fluids.
As you will be having sedation for this procedure, you will be asked to confirm that you have a responsible adult to escort you home when you are ready for discharge. You must also have a responsible adult with you at home for 24 hours following the procedure.
The test and possible complications will be explained so that you understand the procedure and any risks involved.
You will then be asked to sign a consent form. By signing this form, you will have agreed to have the therapy performed and that you understand why it is needed. This does not take away your right to have the procedure stopped at any time.
For the time that you are in the department we want to provide a safe, supportive and pleasant environment. Please do not be afraid to ask if you have any worries or questions at this stage.
For this procedure you will not need to remove your clothes but ties may need to be loosened and shirts opened if they are tight at the neck.
Please remember that your appointment time is not the time you will have your procedure. There will be a wait between your admission and having your test done.
A nurse or doctor will escort you into the room where your procedure will take place. A nurse will stay with you throughout the test.
The Endoscopy Units at Cheltenham General and Gloucestershire Royal Hospitals are training centres.
This means that there may be Registrars and Nurse Endoscopists performing the procedure under the supervision of an experienced endoscopist. Students may also be observing the procedures. Please let the admitting nurse know if you have any concerns about this.
Sedation or throat spray
Intravenous sedation and local anaesthetic throat spray can improve your comfort during the procedure. Intravenous sedation will make you lightly drowsy and relaxed, but not unconscious (asleep).
Anaesthetic throat spray
Throat spray is a local anaesthetic spray used to numb the throat. The throat spray has an effect very much like a dental injection.
Intravenous sedation
Sedation will be given though a cannula (thin tube) inserted into a vein in your hand or arm. This will make you feel lightly drowsy and relaxed but not unconscious (asleep). You will be in a state called conscious sedation. This means that, although drowsy, you will still hear what is said to you and therefore will be able to follow simple instructions during the procedure. You will be able to breathe normally throughout the procedure.
While you are sedated we will check your breathing and heart rate so changes will be noted and dealt with accordingly. For this reason, you will be connected by a finger probe to a pulse oximeter which measures your oxygen levels and heart rate during the procedure. Your blood pressure will also be recorded. Oxygen will be given to you via a mask or a small sponge inserted into your nostril.
Please note that when having sedation, you are not allowed to drive, drink alcohol, operate heavy machinery or sign any legally binding documents for 24 hours following the procedure. You will also need someone to accompany you home and a responsible adult to stay with you for 24 hours.
The procedure
In the examination room any dentures will be removed and a local anaesthetic spray will be applied to the back of your throat to numb it ready for the procedure.
Once you are in a comfortable position on the trolley, a plastic mouth piece will be put between your teeth or gums if dentures have been removed. This helps to protect your teeth and the gastroscope. If you have chosen to have sedation you will then be given the sedation into a vein through a cannula in your hand or arm. The sedation will be allowed to work for a couple of minutes and then the procedure will commence.
The tube will then be inserted through the mouth piece. When it reaches the back of the throat you may be asked to swallow to help the tube go down into the stomach. This will not interfere with your breathing.
Some air will be passed through the instrument to inflate the stomach and allow a clearer view. You may feel wind like discomfort and belch some air up during the test. Please do not be embarrassed.
Any saliva in your mouth will be removed using a small suction tube. When the gastroscope is taken out most of the remaining air in the stomach will also be removed. The required therapy will dictate how long the whole procedure will take. This could be anything between 15 minutes to one hour. Your admitting nurse should be able to advise you on this.
Possible complications and risks
Sedation can occasionally cause problems with breathing, heart rate and blood pressure. If any of these problems do occur, they are normally short lived. Careful monitoring by a fully trained endoscopy nurse makes sure that any potential problems can be identified and treated rapidly. Older patients and those who have health problems, for example, people with breathing difficulties due to a bad chest may be assessed by a doctor before being treated.
Minor complications with sedation happen in less than 1 in every 200 examinations. A few people are excessively sensitive to the sedation we use and become too sleepy. This effect can be rapidly reversed with another injection.
Major complications with endoscopies are very rare (less than 3 in 10,000) and death arising from these is extremely rare (less than 1 in 30,000).
The main serious complication is perforation (a tear) of the oesophagus (gullet) or bowel, which may need an operation and a stay in hospital.
This complication is more common if a dilatation is performed for narrowing of the oesophagus (less than 1 in 200).
If RFA is performed the perforation risk is 1 in 100.
If EMR is performed 1 in 100 may cause bleeding.
If banding is performed, in less than 1 in 100 cases bleeding can be started.
After the procedure
After the therapeutic gastroscopy is completed the nurse, caring for you during the procedure, will take you from the endoscopy room to the recovery area.
Your pulse and blood pressure will be monitored as needed. This is called the recovery period. You may feel a little bloated or have some discomfort in your lower abdomen after the test. You will need to stay in hospital for a couple of hours after the procedure depending on how you recover from the sedation.
Normally you do not see the person who performed your procedure before going home.
Your nurse will go through your report before you are discharged.
It is a good idea to have someone with you at this discussion as many people find they forget what has been said to them due to the sedation.
Going home
It is essential that someone takes you home and that there is a responsible adult to stay with you for 24 hours.
For this period of time, you should not:
- Drive a car, motorbike or ride a bicycle
- Drink alcohol
- Operate machinery or do anything requiring skill or judgement
- Make important decisions or sign any documents A discharge advice leaflet incorporating this information will be given to you before you leave the unit.
Contact information
Appointment Enquiries (answerphone)
Tel: 0300 422 6350
Monday to Sunday, 8:00am to 4:00pm
Medication Advice Line (answerphone)
If you have any questions relating to your medication, please ring the number below for the hospital you will be attending and leave a message. A member of staff will return your call normally within 24 hours.
Cheltenham General Hospital
Tel: 0300 422 3370
Monday to Friday, 8:00am to 6:00pm
Gloucestershire Royal Hospital
Tel: 0300 422 8232
Monday to Friday, 8:00am to 6:00pm
Saturday to Sunday, 9:00am to12:00 Midday