Total Laparoscopic Hysterectomy (TLH)
Hysterectomy can be carried out abdominally, vaginally, laparoscopically or in a combination of these routes. This page gives you information about having a laparoscopic (keyhole) route of surgery called Total Laparoscopic Hysterectomy (TLH) and answers some of the commonly asked questions.
On this page
-
What is a TLH?
-
Why am I having a TLH?
-
Benefits of keyhole hysterectomy
-
Before surgery
-
Pre-operative assessment
-
Will I have to sign a consent form?
-
When should I stop eating and drinking?
-
Day of your surgery
-
During the surgery
-
Risks and complications following surgery
-
After the surgery
-
Will I need a catheter (tube for urinary drainage)?
-
When can I resume my normal diet?
-
How long will I be in hospital?
-
Follow up
-
Going home
-
Recovery and returning to normal
-
When can I go back to work?
-
What about my sex life?
-
When can I drive?
-
Smear test
-
Will I need hormone replacement therapy (HRT)?
-
Further information
-
Contact information
What is a TLH?
TLH is a major gynaecological surgical procedure performed under general anaesthetic (while you are asleep). It involves removing the womb (uterus) and the neck of womb (cervix) using keyhole (laparoscopic) surgery, that is introducing key hole instruments through your belly button and tummy wall. Ovaries and fallopian tubes may or may not be removed, depending on the reason for your surgery. This should have been discussed with you when the decision for surgery was made.
If the ovaries are removed before your natural menopause, you will start the menopause (change of life) immediately after surgery, and depending on your age and medical conditions you will be given advice about taking hormone replacement therapy (HRT) after surgery. HRT may not be suitable for all patients, this will depend on your medical condition(s) and risk factors.
TLH may be combined with other procedures, such as repair of a vaginal prolapse or removal of pelvic lymph nodes if surgery is being performed to treat a cancer. These additional procedures will have been discussed in detail with you by the surgeon during decision making process.
As compared to open or abdominal route surgery, TLH may reduce your recovery period (including hospital stay). It may also reduce the pain and discomfort you experience after the surgery but can have a higher risk of complications, particularly urinary tract injury which may need further investigations and treatment as necessary.
Why am I having a TLH?
Hysterectomy is usually considered as a last resort, usually after other treatments have failed unless performed for certain lifesaving conditions such as cancer. Common reasons for TLH surgery include painful or heavy periods not responding to medical treatments (such as the hormone pill, hormone releasing coil, ablation treatment (burning of lining of womb), pelvic pain secondary to conditions such as endometriosis or adenomyosis, fibroids, endometrial or early-stage cervical cancer. Your doctor will explain why you are having this surgery and a shared decision will be made between you and your doctor.
Benefits of keyhole hysterectomy
- Less pain after surgery than having ‘open’ (traditional) surgery.
- Fewer wound complications.
- Less disruption to your bowel and bladder function.
- Lower risk of Deep Vein Thrombosis (DVT).
- Shorter recovery period and hospital stay compared to other routes of hysterectomy surgery.
Before surgery
You should carry on taking your usual medications, unless told otherwise. We strongly advise that you stop smoking before your surgery. If you are taking the HRT, you may be advised to stop 4 weeks before the surgery, depending upon type and route of HRT you are receiving and risk factors in your case.
If TLH is being performed due to fibroids, then your doctor may discuss some medications to be taken for a few months prior to surgery. This will help shrink the size of the fibroids before your surgery date.
If you develop an illness before your surgery or have any questions about the surgery, please contact the admissions team.
Pre-operative assessment
You will be invited to the hospital any time up to 4 weeks before your surgery date for a pre-operative assessment. During this assessment, we will check your fitness for general anaesthetic and the surgery. This will include recording a full medical history, any current medication and arranging any investigations required. Please tell the nurse practitioner or doctor if you have had problems with any previous surgery, anaesthetic or if you have any allergies – this is very important. This may require a formal anaesthetic review before the surgery.
Your admission details will be confirmed by admissions team by telephone call first and once accepted by yourself, a confirmation letter will follow to confirm the date and place of surgery.
Will I have to sign a consent form?
You will be asked to sign a form on the day of your surgery, giving your consent to undergo surgery. The consent form gives your gynaecologist the right to do only what is written on this form.
The only exception to this is if during the surgery there is an unforeseen problem. You have then consented to have this corrected, for example repair of any injuries, blood transfusion and need to convert the keyhole procedure into open procedure. Please feel free to ask any questions and your concerns about the surgery that you do not understand before signing the consent form.
The medical terms commonly used on the consent form are:
- Total Laparoscopic Hysterectomy (TLH) - removal of the womb which includes the cervix (neck of the womb)
- Oophorectomy - removal of one ovary
- Bilateral oophorectomy - removal of both ovaries
- Salpingectomy - removal of one fallopian tube
- Bilateral salpingectomy - removal of both fallopian tubes
- Salpingo-oophorectomy - removal of one ovary and fallopian tube
- Bilateral salpingo-oophorectomy - removal of both ovaries and fallopian tubes
When should I stop eating and drinking?
Detailed instructions will be included in your admission letter about this. It is very important that you follow the instructions otherwise your surgery may need to be cancelled on the day and another date arranged.
Day of your surgery
An anaesthetist and your surgeon (or a senior member of the team) will see you and go through the consent form. When they are sure that you understand why you are having this procedure and what it involves you will be asked to sign the consent form if it has not already been signed. The anaesthetist and surgeon will also answer any questions or concerns you may have.
We want you to fully understand why you are having the surgery and what the possible risks are. These should have already been discussed with you in the clinic when the decision for surgery was made.
During the surgery
TLH is normally carried out under a general anaesthetic (while you are asleep). Sometimes the anaesthetist may discuss with you the option of spinal or epidural anaesthetic, in addition to general anaesthetic.
A narrow plastic tube (called a cannula) will be inserted into a vein in your arm or hand using a needle. This is used to give you fluids and medications.
After you have been given a general anaesthetic and you are asleep, your bladder will be emptied using a catheter. An instrument will then be inserted through your vagina into the cavity of the womb to help the uterine manipulation required for the laparoscopic hysterectomy.
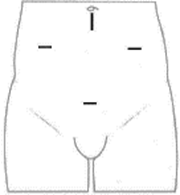
A small cut (about 1 cm) will be made which is usually around your navel (belly button). The abdomen is then filled with gas and an optical instrument, called a laparoscope, will be inserted to allow the internal organs to be viewed before 2 to 3 further small cuts, about 0.5 to 1 cm each, are made on your abdomen. These cuts are used for other instruments to be inserted to perform the surgery. The location of these cuts is decided by the type of procedure and preference of the surgeon so as to increase the safety and efficiency of your surgery.
Your ovaries and fallopian tubes may or may not be removed depending on the reason for your surgery. In most cases the uterus and cervix are removed through the vagina. If the uterus is too large to remove vaginally, or the vagina is too narrow, a slightly larger cut will be made on your abdomen for it to be taken out.
Sometimes a narrow tube or a drain may be left inside your tummy during the surgery. This is usually used for overnight observation to detect any ongoing bleeding. The drain will be secured using a stitch and is usually taken out after a medical review the following day.
The wounds will be closed with dissolvable stitches.
The procedure takes about 1 to 2 hours but you can expect to be in theatre and the recovery area for 3 to 4 hours.
Risks and complications following surgery
- Inflammation, infections and bruising to any wound on the abdomen or in the vagina.
- Haematoma (blood collecting in the wound).
- Return to theatre because of bleeding.
- Chest infection.
- Urinary tract infections such as cystitis may happen in about 1 in every 6 women.
- Vaginal discharge.
- Vaginal vault dehiscence ie separation of incision at the top of vagina which was previously closed at the time of hysterectomy
- Feeling of a bloated tummy.
- Hernia at the site of insertion of the key hole instruments.
- Adhesion (tissue sticking together).
More serious risks
- Injuries to the bladder, ureters (narrow tubes between the bladder and the kidneys), bowel or blood vessels, requiring further investigations or surgery, blood transfusion or longer admission.
- Blood loss can sometimes be heavy during the surgery and this may mean that you need a blood transfusion or use of cell salvage which uses your own blood lost at the surgery and is given back to you after being filtered and washed.
- Anaesthetics carry a small risk and you will be asked by your doctors, before the surgery, about any medical problems that might increase those risks.
- Thromboses (blood clots in the leg or chest) are uncommon after this surgery. Preventative treatment will be discussed and you will be given blood thinning injections during your stay in the hospital. Your doctor will discuss with you if blood thinners are needed for a longer period.
After the surgery
You will normally wake up in the operating theatres recovery area, but you may not remember much until you are back on the ward in your own bed. You will have been given medication during your surgery to relieve the pain when you wake up. You may have some discomfort following your surgery but we will try to control this in the best way possible using a variety of pain relief.
Will I need a catheter (tube for urinary drainage)?
The catheter is usually removed after the surgery (in case of day case procedures) or the day after your surgery as an inpatient. The ward team will check that you are able to pass urine satisfactorily following the removal of the catheter and before your discharge from the hospital.
When can I resume my normal diet?
You may be able to drink a few hours after the surgery, until then you will have a drip into your cannula to provide you with fluids to keep you hydrated. You will usually be eating and drinking normally within a day of the surgery.
How long will I be in hospital?
You will be discharged 1 or 2 days after the surgery. If you have had additional surgery, you may be in hospital for a longer period.
If you have any concerns about going home after the surgery, please discuss these with the staff at the Pre-operative Assessment Clinic.You will be usually discharged the day after your surgery. If you have had additional surgery or any complications during the procedure, you may be in hospital for longer. If surgery was planned as a day case procedure, then you may be allowed to go home the same day - this will have been discussed with you when the discission for surgery was made. If you have any concerns about going home after your surgery, please discuss these with your doctor and the staff at the Pre-Operative Assessment Clinic.
Follow up
You may be given a follow-up appointment at the hospital or you will be asked to make an appointment to see your GP if needed. A routine post-operative hospital follow up appointment may not be needed. Your surgeon will write to you with any results of investigations carried out at the time of your surgery, such as detailed examination of any tissue removed.
Going home
You may still have some discomfort when you leave hospital but you will be given a supply of pain relief medication which you should take regularly for the best effect. You may also be given some laxatives to take home as minor bowel problems such as constipation are common after hysterectomy.
After the surgery, you may experience ‘wind pains’ from having medical air inside your abdomen, these should stop within a few days. Drinking a small amount of peppermint oil in warm water can help. Peppermint oil can be bought in supermarkets and health shops.
You may notice some weight gain during the first few weeks following surgery this is because you are less active. Hysterectomy itself does not cause weight gain.
You may have some light vaginal bleeding (spotting) for up to 6 weeks after the surgery, this is normal. If the bleeding becomes heavy, has a bad smell or if you are concerned, please contact your GP. We advise you not to use tampons but to wear sanitary pads.
If you have any concerns regarding the healing of your skin such as any sign of inflammation or infection, please make an appointment to be seen by your GP. You may need antibiotics if infection is thought to be the cause. It is advised that you keep your wounds clean and dry until healed.
Recovery and returning to normal
You may feel more tired in the weeks following your surgery if you do too much. You may also experience a slight aching discomfort at the wound sites. In some cases, this can carry on for some months after the surgery but most women are able to resume light activities within the first few days after TLH.
It is advisable not to carry out any high impact activities and exercises or lift heavy weights for 6 to 8 weeks, including sexual intercourse. Swimming should be avoided until all the external wounds have healed and any vaginal discharge has cleared up.
It is also advised that you do gentle pelvic floor exercises to support and strengthen your pelvic floor and to prevent prolapse.
When can I go back to work?
We suggest that you stay off work for 4 to 8 weeks; this depends on the nature of your job. We are able to give you an initial sick note for 4 weeks but if you need any longer off work, then you will need to see your GP.
What about my sex life?
The area at the top of the vagina where the cervix was, will have dissolvable stitches which will need about 6 to 12 weeks to heal fully before intercourse can be resumed. You will tend to know when you feel ready to resume intercourse. You should find that there is no alteration in the sensation but you may at first feel slight discomfort. If you experience any pain, please seek advice from your GP.
When can I drive?
You should not drive until you feel able to perform an emergency stop comfortably and are not taking regular pain medication. This usually means about 6 to 8 weeks without driving. We recommend you discuss this with your insurance company.
Smear test
If you had a total hysterectomy (removal of womb and the neck of womb ie cervix) and the detailed examination of tissues did not show any abnormality in the cervix, then you will not need any further cervical smears in future. Your consultant will advise you if smear test from vaginal vault is needed in the future.
Will I need hormone replacement therapy (HRT)?
HRT will have been discussed with you in the Out-patient Clinic before your surgery. Whether or not HRT is offered to you will depend on if your ovaries were removed during the surgery, your age at the time of removal, if you were already postmenopausal and other medical conditions and risk factors.
- If you have not yet reached the menopause and your ovaries are left in place, there is a possibility that they may stop working at an earlier age than normal. If you do develop hot flushes or other menopausal symptoms before the age of 45 you should seek advice from your GP about the possible need for HRT to prevent osteoporosis (premature thinning of the bones).
- If your ovaries are removed at the time of hysterectomy, before your natural menopause, this will bring forward permanent menopause. You will usually be offered an oestrogen replacement therapy until the age of natural menopause ie 50. However, this will depend on your diagnosis, your risk factors and any contraindications to HRT in your case. Your gynaecologist will advise you on the type and dose of HRT. This will be continued and reviewed by your GP. Also, it is important to know that HRT may not address your menopausal symptoms completely, especially the symptoms of hot flushes, night sweats and sexual desire or lack of libido.
- If you have already reached the menopause before your surgery your need for HRT will not change. If you were not taking it before the surgery, you should not need it afterwards.
- You may wish to have a discussion about the advantages and possible disadvantages of HRT with the gynaecology team or with your GP before, or shortly after your surgery.
- If it has been decided that you will need HRT after your surgery you will be given a month’s supply to take home, after that further supplies can be obtained from your GP. Transdermal HRT preparations of oestrogen such as patches, gel or spray, carry minimal risks and can be started soon after your surgery, once you are mobile.
- It is important to know that HRT may take time to show its full benefits. It is usually started on smaller doses and can be gradually increased to the maximum recommended dose so as to address your symptoms.
Further information
We recommend that you read information about menopause and HRT by visiting following - (References from– NICE, British menopause society (BMS).
Menopause Matters
www.menopausematters.co.uk/menopause.php
Menopause exchange
The Menopause Charity
https://themenopausecharity.org
The Daisy Network
Women’s health concern
Menopause Mandate
Health Talk
Seeking information about people’s experience of menopause, visit @healthtalk
Contact information
If you have any problems or concerns after going home, please contact your GP for advice.