Vulvectomy
This page gives you information about having surgery for vulval cancer and answers some of the commonly asked questions.
On this page
-
What is the vulva?
-
What is a vulvectomy?
-
Before surgery
-
Pre-operative assessment
-
Types of vulval surgery
-
Sentinel node biopsy
-
When should I stop eating and drinking?
-
Day of your surgery
-
During your surgery
-
How long will I be in hospital?
-
Pain
-
Catheter
-
Drains
-
Wound healing
-
Possible risks and complications
-
Sexuality
-
At home
-
Diet
-
Constipation
-
When to contact your GP
-
When can I drive?
-
Follow-up
-
Contact information
-
Acknowledgement
What is the vulva?
The vulva is the area of the skin between a woman’s legs which protects the female external genitalia. It has two outer lips called labia majora which surrounds two inner lips called labia minora. The clitoris is just above the opening of the urethra (water passage). The groin area is where the skin creases on the top of each leg. The groin area contains glands/nodes, which are part of the lymphatic system. These filtrate body fluids and can become swollen if they are affected by infection or cancer. It is important to know if the cancer has spread to the lymph nodes, as this helps the doctors decide if you need more treatment.
What is a vulvectomy?
Women with vulval cancer will need surgery to remove the affected area of vulval skin. Surgery is the main treatment for vulval cancer. The aim of the surgery is to remove both cancer and a border (margin) of normal tissue around it. Surgery may be given alone or in combination with chemotherapy and radiotherapy. The lymph nodes in one or both groins may be removed during the surgery. The type and extent of vulval surgery will depend on the size and position of the cancer. Surgery is decided on an individual basis.
Before surgery
You should carry on taking your usual medications, unless told otherwise. We strongly advise that you stop smoking before your surgery.
If you develop an illness before the date of your surgery, or if you have any questions, please contact your consultant’s secretary.
Pre-operative assessment
You will be invited to the hospital any time up to 2 weeks before your surgery for a pre-operative assessment. During this assessment we will check your fitness for general anaesthetic and surgery. This will include recording a full medical history, your current medication and arranging any investigations needed. Please tell the nurse practitioner or doctor if you have had problems with any previous surgery or anaesthetic, or if you have any allergies – this is very important.
At this visit you will have the opportunity to discuss what to expect before, during and after your surgery. Your admission date should also be confirmed.
You will be asked to sign a form giving your consent to the surgery. The consent form gives your gynaecologist the right to do only what is written on this form. The only exception to this is if during the surgery there is an unforeseen problem, you have then consented to have this corrected. Please feel free to ask any questions about the surgery that you do not understand before signing the consent form.
Types of vulval surgery
Figure 1 shows a partial vulvectomy where the cancer is on one side of the vulva.
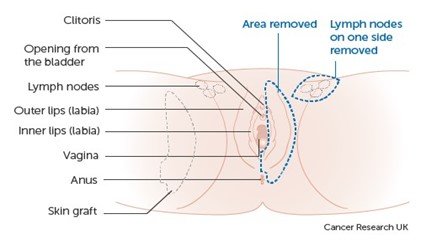
Figure 2 shows a partial vulvectomy where the cancer is at the top of the vulva.
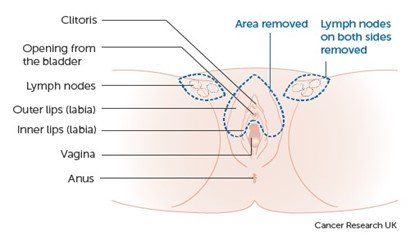
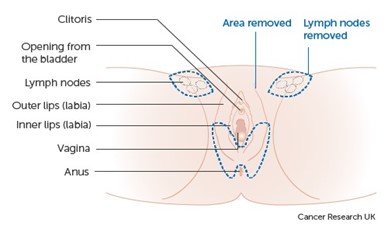
Figure 3 shows a partial vulvectomy where the cancer is in the lower part of the vulva.
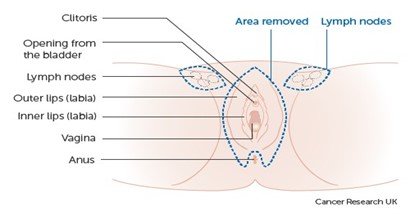
Surgery to remove the whole vulva is called a radical vulvectomy or vulvectomy (see Figure 4). The surgeon removes the whole vulva, including the inner and outer lips of the vulva. You may have the clitoris removed as well.
Sentinel node biopsy
This is performed at the same time as the vulval surgery. For this test, the surgeon removes the sentinel node (or nodes). The sentinel node is the first node that fluid drains to from the vulva. This means it is the first lymph node the cancer could spread to. If this node does not contain cancer, it is unlikely that further lymph nodes will contain cancer cells.
To find the sentinel lymph node a dye or small amount of a weak radioactive chemical (called a tracer) is injected into the area around the cancer. The dye or radioactive tracer follows the route of the fluid that drains from the vulva to the lymph nodes; the first lymph node that the dye or tracer reaches is the sentinel node.
When should I stop eating and drinking?
Detailed instructions will be included in your admission letter about this. It is very important that you follow the instructions otherwise your surgery may need to be put off until a later date.
Day of your surgery
An anaesthetist and your surgeon (or a senior member of the team) will explain to you what will happen during your operation.
We want you to fully understand why you are having the surgery and what the possible risks are.
You will be asked to sign a consent form if you have not already done so and you will have the opportunity to ask any questions that you may have.
If you are having a sentinel lymph node biopsy an anaesthetic cream will be applied to the vulval cancer and 4 injections of a radioactive substance will be given into this area. You will then be taken to the CT scanning department for a number of scans before the surgery.
During your surgery
A vulvectomy is normally carried out under a general anaesthetic (while you are asleep). A narrow plastic tube called a cannula is inserted into a vein in your arm or hand using a needle. This tube is used to give you fluids and medications. After you have been given a general anaesthetic and you are asleep, a catheter (a tube for urine drainage) may be inserted into your bladder. After the surgery the wound will be closed with dissolvable stitches. The procedure will take 2 to 3 hours, but you can expect to be in theatre and recovery for 3 to 4 hours.
How long will I be in hospital?
This will depend on the type of surgery you have had, your recovery and your home circumstances.
Pain
You will be given medication during your surgery to relieve the pain when you wake up.
You may have some discomfort following your surgery but we will try to control this in the best way possible using a variety of pain relief. Depending on the extent of your surgery, you may need strong pain relief, such as morphine, for the first few days following the operation. Morphine may be given through a Patient Controlled Analgesia (PCA) pump. If you have a PCA pump it will be attached to a cannula (fine tube) which is placed in a vein in your arm. You can control the pump yourself using a handset which you press when you need more pain relief.
Catheter
The length of time that the catheter will stay inside your bladder will depend on the type of surgery you have had.
Drains
If you have had some groin lymph nodes removed then you might also have some drains (tubes) in place. These tubes will help to drain away the lymph fluid and can remain in place for a number of days. You may not need to stay in hospital while you have a drain in place.
Wound healing
You will not have any dressings covering your vulval wound; normally a sanitary pad is used. Any stitches you have will be dissolvable.
It is important that you keep the wound area clean and dry to help with healing and to prevent infections. Shower the wound area with lukewarm water and dry with a non-shedding cloth or cool hair dryer a minimum of 3 times a day or every time after going to the toilet. Do not use a hairdryer in your bathroom.
Possible risks and complications
- Bleeding during and after your surgery may result in you needing a blood transfusion.
- Infections - to reduce the risk you may be given antibiotics during and after your surgery.
- For some women it may take a few weeks for the wound to heal.
- Deep Vein Thrombosis (DVT), Pulmonary Embolism (PE) (blood clots in the legs or lungs) - you will be asked to wear special stockings during your stay in hospital. This is to help prevent any blood clots forming. You will be given daily blood thinning injections for 28 days following your surgery.
- Injuries to local structures such as nerves, blood vessels, anal sphincter and the urethra.
- Some women can have difficulty with emptying their bladder following vulvectomy and may need to go home with the catheter in place. This will only be for a few days. If this is the case you will be shown how to care for the catheter.
- Further surgeries and other treatments.
- Risk from the general anaesthetic.
- Lymphoedema, swelling in the lower body or legs. This can be permanent and happen months or years after the surgery. Your nurse specialist or GP will refer you to Lymphoedema Services.
- Lymphocyst swellings may develop after your surgery. They can often be naturally reabsorbed by your body or they may need to be drained by your surgeon.
Sexuality
If you are sexually active it may be some months before you really begin to enjoy sex again. Do not be surprised if you feel very unsure about it. Remember that you need to look after yourself and allow yourself time to heal. Talk to your partner if you have one, and be as honest as you can about what you want and do not want. It is fine to say no to any kind of sexual contact that does not feel right.
We can offer psychological support if you need it.
At home
The following information is a guide to help with your recovery:
- You may still have some discomfort when you leave hospital but you will be given a supply of pain relief medication which you should take regularly for the best effect.
- You may feel weak or tired, this may last for a few days or weeks and you might feel that you need to rest more than usual.
- Avoid wearing tight clothing and using any lotions or perfumes in the area of your operation.
- Do not do too much walking until the skin has healed comfortably.
- Do not have full penetrative intercourse for 6 to 8 weeks so that the wound has time to heal.
- You should avoid the use of tampons for 6 to 8 weeks to prevent infection to the wound area.
- It may be arranged for a district nurse to assess your wound once you are home. They will carry out wound care if needed.
- It is normal to feel a tingling and pulling feeling around the area of the surgery as your wound goes through stages of healing. It may take some time for the wound to heal completely.
- Although vulval stitches are dissolvable they can become tight. These can be removed by the district nurse after 10 days, depending on how well the wound has healed. If you are experiencing discomfort and stinging when passing urine this is usually due to the acidity of urine coming into contact with the wound. Pouring a jug of lukewarm water over the wound while sitting on the toilet might ease your discomfort.
- Due to the location of the wound, it is common that the wound may show signs of infection despite frequent washing and your best efforts to keep the wound clean. If you experience any redness, heat or offensive smelling discharge from your wound you should to speak to the district nurse or your GP. They may take a swab from the wound and test for infection. It is likely that they will prescribe you a course of antibiotics.
- At first you may have a brownish discharge, this is normal. If the discharge gets heavier, foul smelling or if you have bright red bleeding, you should contact your GP or specialist nurse.
- If you are still having periods your next period may be early or late as surgery can upset your normal cycle. It can take a while for your cycle to settle back into a normal pattern.
- If you work, you may return 2 to 6 weeks following the surgery. This will depend on the depth and size of the wound, healing, your general health and the type of job you do.
- Gradually increase your activity each day. Some exercise is important because sitting for long periods can cause ankle and foot swelling and increase your risk of Deep Vein Thrombosis. Walking is an excellent way to exercise. Gradually increase the length of your walks, but only walk a distance you are comfortable with.
- Do not go swimming until your vaginal bleeding has stopped and your wound has healed completely.
Diet
Try to eat a healthy balanced variety of foods with plenty of fresh fruit and vegetables. Introducing high fibre food including wholemeal bread, bran flakes, beans and pulses along with plenty of fluids will help prevent constipation. You should drink at least 8 glasses of water (or non-sugary drinks) every day. Protein rich foods including fish, eggs, meat, hearty green vegetables and beans and pulses will help with the healing process. Avoiding fatty foods, excessive alcohol, cakes and sweets will help you to avoid putting on weight while you are less active. It is advisable to control your calorie intake. The operation will not make you put on weight.
Constipation
Pain relief medication, reduced activity, having an operation and changes in your appetite can all affect your bowel function. If you are constipated following your discharge from hospital it is important that you try to address it as soon as possible
You should try to increase your fluid intake and eat a well-balanced diet with foods rich in fibre such as wholemeal bread, bran flakes, beans and pulses.
If you have not moved your bowels for 3 days, please contact your GP or district nurse who may give you some medication to help.
When to contact your GP
Seek medical attention if you have any the following:
- Severe pain not controlled by pain relief medication.
- Fever, shaking, chills or other signs of a fever.
- Signs of wound infection such as increased redness, swelling, tenderness, warmth or drainage from the wound.
- Offensive smelling discharge.
- Excess bleeding.
- Persistent vomiting, unable to tolerate food and fluids
- Severe pain in either calf or leg, sudden shortness of breath or chest pain.
- Problems passing urine and/or other urinary problems.
When can I drive?
You will be able to travel as a passenger, but if you are travelling long distances, please make sure that you stretch your legs regularly.
You should not drive until you feel able to perform an emergency stop comfortably and are not taking regular pain relief medication. This usually means about 6 weeks before starting to drive again, but it is advisable to discuss this with your insurance company.
Follow-up
Results and treatment plans will be discussed at our weekly multi-disciplinary team meeting (MDT). These will then be discussed with you and the appropriate follow up actions arranged.
Contact information
If you need more information or would like to talk to a member of the team, please telephone one of the numbers listed below.
Gynaecological Cancer Nurse Specialists
Cheltenham General Hospital
Tel: 0300 422 3181
Gloucestershire Royal Hospital
Tel: 0300 422 6669
If your call is not answered, please leave a message and one of the Gynaecological Cancer Nurse Specialists will contact you by the end of the next working day.