Laparoscopic Hysteropexy
This page gives you information about uterine prolapse and laparoscopic hysteropexy (also known as sacrohysteropexy). This procedure is performed for women who wish to have uterine preservation surgery for their prolapse.
On this page
-
What is prolapse of the uterus/vaginal apex?
-
About laparoscopic hysteropexy and the mesh used
-
Why mesh is used and what is the difference with vaginal meshes?
-
What conditions lead to uterine prolapse?
-
What are the symptoms of prolapse?
-
What are the alternative non-surgical treatments?
-
What are the benefits of laparoscopic hysteropexy?
-
Are there any risks with this operation?
-
Complications which may occur due to the mesh
-
What are the concerns with synthetic meshes?
-
What will happen before the operation?
-
What will happen when I come into hospital?
-
How will the hysteropexy be carried out?
-
Vaginal repair
-
What happens after the operation?
-
When can I return to my usual routine?
-
Follow up
-
Cervical smears
-
Contact information
-
Further information
What is prolapse of the uterus/vaginal apex?
A prolapse occurs when one or more of the pelvic organs, (uterus, bladder, and bowel), the pelvic floor muscles, vaginal walls, or their attachments (ligaments) become weak. This causes the pelvic organs and/or vaginal walls to bulge downwards (herniate) into the vagina or in more severe cases, outside of the vagina.
Apical vaginal prolapse is a prolapse from the top of the vagina. The apex is the deepest part of the vagina where the uterus is usually located.
A uterine prolapse is often accompanied by a weakness and prolapse of the walls of the vagina such as a rectocele (a bulge of the back wall of the vagina) or a cystocele (prolapse of the front wall of the vagina). Sometimes further vaginal surgery is required to correct the prolapse at the same time as the hysteropexy procedure. Your surgeon will discuss this with you.
About laparoscopic hysteropexy and the mesh used
This procedure is performed in women who develop prolapse of the uterus (womb) and wish to have this repaired without having a hysterectomy (removal of the uterus).
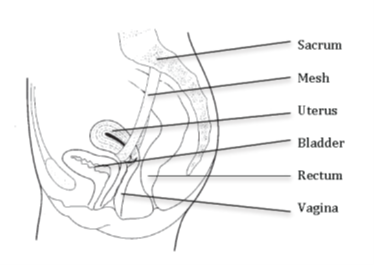
Hysteropexy corrects the prolapse using a strip of permanent synthetic (man-made) mesh to lift the uterus and hold it in place. The mesh material is made of woven polypropylene or Prolene (a net like type of plastic). One end of the mesh is attached to the cervix (neck of the womb) and the other to the ligaments over the sacrum (base of the lower back). This will support the uterus and prevent it from prolapsing down.
The operation is performed under a general anaesthetic (while you are asleep) through laparoscopic (keyhole) surgery.
Why mesh is used and what is the difference with vaginal meshes?
In this operation, the mesh reinforces the support that would usually be provided by your own connective tissues or ligaments (attachments). In the event of prolapse, these forms of natural support have become damaged or weakened, so can no longer hold the skin or organ in its normal position.
You might have heard about the mesh problems that occur when mesh is used in the walls of the vagina or around the bladder through a cut in the vagina. Although this is the same type of mesh, it is placed through an abdominal (tummy) technique and it is considered to be safer with a reduced complication risk compared to vaginal mesh insertion. Your doctor will discuss this with you.
What conditions lead to uterine prolapse?
Prolapse happens over a period of time, to varying degrees. There are usually multiple factors in the development of prolapse. These can include childbirth, abnormally weak collagen, being overweight, heavy lifting, chronic constipation, smoking or a lack of hormones after the menopause.
Many women will have a prolapse of some degree after childbirth; it is not unusual and unless you have symptoms, you do not need to seek treatment.
What are the symptoms of prolapse?
Symptoms may vary depending on the type and severity of prolapse. Usually, symptoms are worse towards the end of the day. In general, the symptoms can include:
- A dragging feeling, heaviness or a lump in the vagina
- Difficulty opening the bowel or bladder
- Difficulty with intercourse or having a loose sensation.
Pain is not usually a symptom of prolapse. Some women with prolapse may not have any symptoms in which case no treatment is required.
What are the alternative non-surgical treatments?
Do nothing
If the prolapse (bulge) is not troubling you greatly then surgery may not be necessary. If, however the prolapse is outside the vagina and exposed to the air, it can become dried out and eventually become ulcerated. Even if it is not causing symptoms, in this situation we would recommend supporting it back inside the vagina with a vaginal pessary (see below).
Pelvic Floor Exercises (PFE)
The pelvic floor muscles form a bowl at the bottom of your pelvis. These muscles support your pelvic floor organs (uterus, vagina, bladder and rectum). Every muscle in the body needs exercising to keep it strong so that it functions properly.
PFE help strengthen the pelvic floor muscles and therefore give more support to the pelvic organs.
These exercises may not get rid of the prolapse completely but they can make you more comfortable and are best taught by an expert (usually a physiotherapist). These exercises have little or no risk and even if surgery is required at a later date, they can help to strengthen the area beforehand. Please discuss with your surgeon for a referral to a physiotherapist.
Vaginal pessaries
Ring pessary
This is a ring made of PVC which is inserted inside the vagina to push the prolapse back up. This usually gets rid of the dragging sensation and can sometimes improve bladder and bowel symptoms. The ring pessary is very popular and needs to be changed every 6 months. This can be done by your GP or practice nurse. We can show you an example of one in clinic, please ask.
Some couples find that the ring pessary can interfere with intercourse, however intercourse is possible. Ring pessaries are not always suitable and do not always stay in place. If this is the case a shelf or Gellhorn pessary may be recommended.
Shelf pessary
This is a different shape pessary which cannot be used if you are sexually active. The shelf needs to be checked every 6 months and is usually inserted in hospital by a specialist nurse or doctor.
Gellhorn pessary
This pessary is made of silicone which is softer than the shelf pessary. The Gellhorn pessary is not suitable for sexually active women. This pessary will also need to be checked every 6 months in hospital by a specialist nurse or doctor.
What are the benefits of laparoscopic hysteropexy?
Hysteropexy preserves the anatomy of the vagina, suspending the uterus in its normal position by reinforcing weakened ligaments with a mesh. This procedure is minimally invasive, with limited disruption to the surrounding organs such as the bowel and bladder.
It also offers a potentially shorter operation time and quicker recovery.
Many women choose hysteropexy because it enables them to keep the uterus. In younger women, this may be influenced by a general desire to feel young, complete and fertile. Many women express relief when they learn that the uterus can be preserved, as in most cases they had assumed that hysterectomy (removal of the uterus) was the only option.
The uterus and cervix can have an important role in sexual function. Sexual well-being may decrease after hysterectomy due to damage to the nerves and supportive structures of the pelvic floor. In some women removal of the uterus may even influence sexual and personal identity.
Although laparoscopic hysteropexy is a relatively new procedure, initial results indicate that it is at least as effective as standard vaginal hysterectomy in curing prolapse.
Are there any risks with this operation?
Hysteropexy is considered major surgery, and as with all surgery, there are associated risks that you need to be aware of when deciding on the right treatment for you. The risks are:
- Wound or bladder infection, which are usually treatable with a course of antibiotics.
- Damage to the bladder or ureters (tubes which drain the kidneys); affecting 1 in every 200 women.
- Damage to the bowel; very rarely encountered with a risk of about 1 or 2 in every 1000 women.
- Excessive bleeding. This may happen during the operation with a risk to about 1 in every 100 women.
- Venous Thromboembolism (VTE), this is when a blood clot forms in a leg vein, or in the lungs, and happens in about 1 in every 250 women. Treatments will be given to reduce this risk.
- Prolapse recurrence. If you have one prolapse, there is an increased risk of having another during your life, especially in the area where no repair was performed. Around 1 in 10 patients will get a recurrence of the same prolapse and 3 in 10 women will require treatment for prolapse of another area at some stage.
- Failure to cure symptoms. It is important to understand that even if an operation is successful in treating your prolapse, it may not relieve all of your symptoms.
- Back pain. As you will be lying on your back with your legs raised during the operation, this can lead to back pain which is usually short lasting. This can occur more commonly if you have a back pain already.
- Bladder emptying or voiding problems. Generally, improves after surgery for prolapse but as is the case for any surgery in the pelvic area there may be problems with voiding (emptying your bladder) after the operation. There can be persistence of voiding problems for many months in 1 in 10 women but very few women will have ongoing difficulty or be unable to void long term.
- Painful sexual intercourse. Once the abdominal wounds are comfortable and there has been no vaginal surgery at the time of hysteropexy; then there is nothing to stop you from having sex. The healing usually takes about 6 weeks. Some women find sex is uncomfortable at first, but it gets better with time. Occasionally, pain during intercourse can be long-term or permanent. Pain during intercourse is less common after this surgery than after vaginal surgery.
Complications which may occur due to the mesh
- Mesh erosion/exposure (wear through to the surrounding tissues or vagina). This is rare with a risk of 2 to 3 per every 100 women. There is also a small risk of mesh erosion into the nearby organs such as the bladder, bowel or vagina. Although this is very uncommon, the treatment depends on where the mesh has worn through and the symptoms it is causing. In some cases, with minimal or no symptoms, close monitoring alone is required. If there is infection, this can be treated with antibiotics. Sometimes an operation to trim part of the mesh is performed, which may compromise the results of the operation. In a small number of more serious cases, an operation may be needed in a specialist centre to remove all or part of the mesh and may also involve an operation on any damaged organs such as the bowel or bladder.
- Infection of mesh. The mesh and/or the tissues attached to it may get infected but this is uncommon. This is usually treated with antibiotics and in rare cases, by removing the mesh. Sometimes, referral to a specialist hospital is needed in order to remove the mesh. Very rarely infection can occur around the bone (sacrum) where the mesh is attached.
- Chronic pelvic pain. In our experience, this is uncommon and less than 2 in every 100 women may experience pain which continues after the wounds have healed. Usually, pain had been present before surgery which has not resolved post operation. Pain is usually managed with pain relief and physiotherapy treatment.
If you need another operation in the future, for example a hysterectomy, mesh inside the abdomen can make this procedure more difficult. The mesh needs to be cut and removed with the hysterectomy. Surgery to remove the mesh can reduce the effectiveness of the original operation and result in the prolapse recurring.
To date, there has been no evidence that autoimmune problems can be caused by meshes.
Changes in bladder and bowel function
Laparoscopic hysteropexy can help to restore the normal position of the bladder and bowel and therefore improve their function. However, in some women the straightening of the vaginal walls when prolapse is repaired can reveal a pre-existing weakness of the bladder neck and lead to a new incontinence problem. If you already have incontinence, this can persist, sometimes get worse or improve after the operation.
Some patients experience worsening constipation following this surgery but this tends to resolve over time. It is important to try and avoid being constipated following surgery to reduce the risk of prolapse recurrence.
Childbirth
If you are planning to have children after the procedure, a pregnancy may damage the repair and cause the prolapse to recur. To help prevent this, you may be advised to have a scheduled caesarean section rather than a vaginal birth.
Abdominal incision (cut)
Although the aim is to perform the surgery through a laparoscope (keyhole incisions), sometimes this is not possible. In this case a laparotomy (wider cut in the abdomen) may be required. In less than 1 in 100 cases, the operation needs to be converted from laparoscopy to laparotomy (abdominal cut) during surgery, especially if there is significant bleeding or damage to surrounding structures.
Laparoscopic hysteropexy is considered major surgery but is a relatively safe operation where serious complications are uncommon.
All surgery has risks so you and your doctor must discuss these and the benefits of surgery, while also considering any alternative treatments.
What are the concerns with synthetic meshes?
There have been problems with mesh used in prolapse and continence surgery which are inserted through a vaginal incision (cut). Although the same material is used in abdominal surgery such as laparoscopic hysteropexy, the mesh complications appear to be much less.
The complications appear to be significantly reduced by stopping the mesh coming in contact with the vagina and other surrounding structures by covering the mesh with a layer of skin that lines the abdomen called the peritoneum. With this technique the risk of mesh erosion/extrusion is reduced.
In a small number of cases, an operation may be needed in a specialist centre to remove all or part of the mesh and may also involve an operation on any damaged organs such as the bowel or bladder.
What will happen before the operation?
Before your admission for surgery, you will be asked to attend a pre-admission clinic to make sure that you are fit and well for your surgery.
You will be seen by a nurse practitioner or a doctor, who will ask about your general health, past medical history and any medication that you are currently taking. Any necessary investigations (for example, blood tests, ECG, chest X-ray) will be arranged. Information about your admission, hospital stay, operation and pre and post-operative care will be given.
You will be given the opportunity to ask any further questions that you may have.
You will also be given a questionnaire that you need to fill in before your operation. This is regarding your symptoms and how it affects you on a daily basis. Six months after your surgery the same questionnaire will be sent to you and the result will be reviewed. If there are any problems we will get in touch with you.
What will happen when I come into hospital?
You will be asked to come in either the day before or the same day as your surgery. An anaesthetist and your surgeon (or a senior member of the team) will explain to you what will happen during the operation including its purpose and the associated risks. You will be asked to sign a consent form, if you have not already done so, and you will have the opportunity to ask any questions not covered during your pre-admission clinic appointment.
How will the hysteropexy be carried out?
The operation is performed under general anaesthetic (while you are asleep). You will have a drip (thin tube) inserted in to a vein in your hand or arm to administer medications. A catheter (a tube for urine drainage) is inserted into your bladder once you are asleep.
There will be 4 small incisions on your abdomen for introducing the camera and the instruments for the operation. After careful dissection, a piece of permanent synthetic mesh (Prolene mesh) is stitched around the cervix (neck of the uterus). The mesh is secured to ligaments over the sacrum (lower backbone). The effect of this is to support the vagina and prevent it from prolapsing (dropping) down, returning it to its correct position. The mesh is covered with a layer of skin inside the abdomen to avoid it coming into contact with surrounding structures. Eventually, new connective tissue grows into the mesh, which forms a new strong ligament and remains permanently in the body.
Vaginal repair
Other types of prolapse may result from stretching and weakening of the walls of the vagina such as cystocele (bulging of the bladder through the front wall) or rectocele (bulging of bowel through the back wall). All of these conditions can result in the feeling of something coming down the vagina.
Following the hysteropexy further repair may be required to correct these types of prolapse at the lower part of the vagina. This may be required during your operation or at a later date. The repair operation tightens the walls of the vagina and the pelvic floor muscles. All the stitches used are dissolvable.
What happens after the operation?
When you wake up from the anaesthetic you will have a drip (thin tube) in the back of your hand to allow fluids and medications to be given.
The surgeon may place a vaginal pack (swabs inside the vagina) to stop any bleeding into the tissues. There will also be a tube in the bladder (catheter) to avoid urinary retention. The pack and catheter is usually removed the day after surgery.
Will I have pain?
Most people experience some pain or discomfort for the first few days after surgery. You will be offered pain relief to help to reduce the discomfort. This may be by injection, tablets or suppositories. You will be encouraged to take pain relief, as being pain-free will help you to recover more quickly.
Due to the anaesthetic, being in pain, and having strong pain relief can sometimes make you feel nauseous or sick. This can be relieved by injections or tablets.
Many women get wind pains a few days after the operation which can be uncomfortable and make the tummy look distended (swollen). This should not last long and can be relieved by medicines, eating and walking about.
Will I bleed?
After the operation, if you had vaginal repair, you may have some vaginal bleeding and you will need to wear a sanitary pad. We advise you not to use tampons. Your vaginal discharge should change to a creamy colour over the next 2 to 3 weeks. If you have any new pain, fresh bleeding, or a bad smelling discharge after you go home, you should contact your GP.
Will I have stitches?
You have some stitches on the small incisions on your abdomen; these normally dissolve 2 to 3 weeks after your operation. If you have had a vaginal repair, you will have vaginal stitches - these are dissolvable. Threads may come away for up to 3 months, this is normal.
How will I cough?
If you need to cough, your stitches will not come undone. You will be wearing a sanitary towel, and coughing will hurt less if you press on your pad firmly to give support between your legs.
When will I go home?
After a laparoscopic hysteropexy most women usually stay in the hospital for 1 or 2 days. Recovery time varies from woman to woman. It is important to remember that everyone’s experience is different, and it is therefore best not to compare your own recovery with that of others on the ward.
When can I return to my usual routine?
Recovery is a time-consuming process, which can leave you feeling tired, emotionally low or tearful. Although the scars from laparoscopic (keyhole) surgery are small, this does not shorten the healing process. The body needs time and help to build new cells and repair itself.
Depending on the surgery you have had and the nature of your work, you will need to take 4 to 6 weeks off work to recover. If you require a sick note, please ask.
Sex after the operation
Healing usually takes about 6 to 8 weeks, so penetrative intercourse is not advised during this period.
Some women find penetrative intercourse uncomfortable at first but it gets better with time and may improve if you use a lubricant, such as vaginal moisturisers, topical oestrogen cream or pessaries.
Do expect things to feel a little different after the operation as the vagina will be suspended and therefore under slight tension. Sometimes, sensation during sex might be reduced and you may find it more difficult to achieve orgasm.
Weight and exercise
Reduced levels of activity and an increase in appetite may add to you putting on extra weight. It is important to continue to exercise following surgery. After 6 weeks you can gradually build up your level of activity, and after 3 months you should be able to return to your usual level of activity. You should try to avoid any unnecessary heavy lifting to reduce the risk of the prolapse recurring.
Low impact exercises such as cycling and swimming are good and have less impact on the pelvic floor.
Follow up
A follow-up appointment will be arranged after surgery to assess your recovery. This will be either as a telephone follow up, clinic appointment or a questionnaire. The clinic appointment will be sent to you through the post.
You should contact your GP or gynaecology team if you notice any of the following:
- An increase in your temperature.
- Warm, painful, swollen leg.
- Chest pain or difficulty breathing.
- Swelling around your wound or tummy.
- Pain that is getting worse.
- Discharge from your wounds or vagina.
- Blood in your urine.
- If you are unable to open your bowel.
Cervical smears
After a hysteropexy you will need to continue to have routine cervical smear tests. If you have any further questions, please feel free to ask your doctor.
Contact information
If you have any problems or concerns after going home, please contact your GP or if out of normal working hours NHS 111 for advice.
Alternatively, you can contact the hospital, either the ward you were discharged from or an Advanced Urogynaecology Practitioner.
Advanced Urogynaecology Practitioner
The Women’s Centre
Gloucestershire Royal Hospital
Tel: 0300 422 6246
Tel: 0300 422 6278
Monday to Friday, 8:00am to 4:00pm
Further information
Patient decision aid about choice of procedure for prolapse of the uterus (NICE)
Sacrohysteropexy for Uterine Prolapse (Womb Prolapse) - British Society of Urogynaecology
https://bsug.org.uk/budcms/includes/kcfinder/upload/files/info-leaflets/SHP-BSUG.pdf
NICE guidelines: Uterine suspension using mesh (including sacrohysteropexy) to repair uterine prolapse
https://www.nice.org.uk/guidance/ipg584
Patient
Website: https://patient.info/womens-health/genitourinary-prolapse-leaflet
Bladder & Bowel UK
Helpline: 0161 214 4591
Monday to Friday, 9:00am to 4:30pm
Email: bbuk@disabledliving.co.uk
Website: www.bbuk.org.uk