Open repair of an Abdominal Aortic Aneurysm (AAA)
This information on this page is for patients and their family to help them understand the important things about having treatment of an Abdominal Aortic Aneurysm (AAA).
On this page
What is an Abdominal Aortic Aneurysm (AAA)?
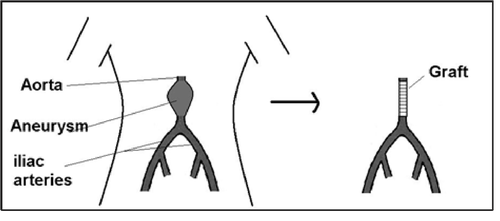
An abdominal aortic aneurysm is a swelling of the aorta which is the main blood vessel (artery) that leads away from the heart. The majority of aortic aneurysms affect the section of aorta in the belly (abdomen).
The decision to operate on an aneurysm that is not causing symptoms depends on its size and the surgical risks involved. Many smaller aneurysms may never require surgery. However, with larger aneurysms an operation is considered if the risk of the aneurysm rupturing is greater than the risk of surgery. Your consultant will discuss the risks with you when considering this operation.
Symptoms
Aortic aneurysms usually cause no symptoms. Occasionally they may cause abdominal or back pain in which case you should seek urgent medical attention.
About the operation
An open repair of an aortic aneurysm is a major operation which involves replacing the aneurysm with a synthetic graft or tube. This may be carried out through a large incision (cut) in the abdomen. The type of operation you have will depend on your general health and the size and shape of your aneurysm. This will be discussed with you by your consultant before the surgery.
Alternative treatment
- Not having surgery is always an option. The risks of having or not having the surgery will be discussed with you at your clinic appointment.
- Endovascular aneurysm repair (EVAR) is minimally invasive surgery performed through small cuts in your groin, the aneurysm is repaired using stent graft that is placed inside the artery to strengthen the aneurysm and prevent it bursting (rupturing).
Benefit of having surgery
- To prevent the aneurysm from bursting in the future. If the aneurysm is not repaired there is a risk of not surviving if the aneurysm bursts.
Risks and complications
- Heart failure or kidney failure.
- Chest infection, infection of the graft or wound.
- Blood clots forming in the legs or lungs (Deep Vein Thrombosis, DVT or Pulmonary Embolism, PE).
- Pressure sores - to reduce this risk the nursing staff will help you to move regularly while you are confined to bed. They will also encourage you to get up and move around as quickly as possible.
- There is around a 2 to 3 in 100 risk that you will not survive the operation. Your overall fitness will affect the success of the operation but your consultant will discuss this with you.
- Your sexual activity may be affected after aneurysm surgery. If you have any concerns about this, please mention it to your consultant.
- Sometime after surgery you may develop weakness (a hernia) around the wound.
- Lower limb ischaemia (a restriction in blood supply) may result in requiring further surgery such as bypass or extremely small risk of limb loss.
- Rare risk of bowel resection due to ischaemia and stoma formation
What to expect
You will usually be admitted to hospital on the day of your operation and will be in hospital from 5 to 10 days depending on the type of operation you have.
After your operation you will be transferred to the Department of Critical Care (DCC) for careful monitoring. This is planned and it is important that your relatives are aware that this is normal procedure.
You will remain in the DCC until you are stable enough to be transferred to a surgical ward. However, if a critical care bed is not available on the day of your surgery, it would be unsafe to carry out your operation. This will mean that you will be discharged home and be given another date for your operation.
While you are a patient in the DCC the physiotherapist will visit you to show you how to do breathing and leg exercises. This is to help prevent blood clots forming you will also be given small daily injections of a medication to thin the blood.
Pain control
You will have some pain and discomfort after your operation and you will be given strong pain relief to help control this.
After the operation pain relief is usually given through a continuous drip going into your back, this is called an epidural. The anaesthetic doctor and a specialist nurse will monitor this closely to make sure that the pain control is working.
Your pain relief will be gradually reduced. When the epidural is removed you will be given pain relief tablets regularly.
Diet and fluids
You may not be able to eat for a few days after surgery, as sometimes the intestine does not work immediately after the operation.
During this time, you will be allowed to drink small amounts of water and will be given fluid through a drip (a tube inserted into a vein in your arm).
You may also have a tube passed through your nose into your stomach when you are asleep during the operation. This is to drain any fluid from your stomach and prevent vomiting. Once you start passing wind the tube will be removed and you will be able to drink larger amounts of fluid and food will gradually be introduced.
Bowel movements and passing urine
You are unlikely to have your bowels open for the first few days after the operation. Once your bowels begin working again you may experience diarrhoea which will usually settle within 24 hours.
A catheter tube will be passed into your bladder during the operation to drain away the urine. This will be removed when you are mobile and able to walk to the toilet.
Wound care
Dissolvable stitches or small metal clips will be used to close your wound(s) which will be checked regularly. The clips will be removed 10 days after your operation by the district nurse; the ward staff will arrange this.
Going home
You will feel weak after the operation but this is normal. Once you are able to move around the ward on your own and you are eating and drinking normally, arrangements will be made for you to go home.
It is important that you have restful periods and gradually build up to your normal activity each day.
Recovery can take several months. You are advised to avoid heavy lifting for 2 months. You can begin driving again when you can perform an emergency stop comfortably and without hesitation. Most patients take about 4 weeks to reach this level safely. We advise you to inform your car insurance company that you have had an operation.
Follow up
You will be seen in the outpatient clinic about 6 weeks after your discharge.
Contact information
If you have any minor concerns before being seen in the follow-up clinic, please contact your GP or the:
Vascular Ward – 4B
Gloucestershire Royal Hospital
Tel: 0300 422 5543
Alternately you can contact your consultant via the hospital switchboard:
Gloucestershire Hospitals Switchboard
Tel: 0300 422 2222
When prompted ask for the operator, then for your consultant.
If you are worried or feel unwell, please contact the Emergency Services (Tel: 999) or attend your nearest Emergency Department.
Further information
More information about aortic aneurysms can be found at the following websites:
National Institute for Health and Care Excellence (NICE)
Website: https://www.nice.org.uk/guidance/ng156/informationforpublic
NHS
Website: https://www.nhs.uk/conditions/abdominal-aorticaneurysm/